


NAMI Western Massachusetts supports NAMI Mass's recent response to antisemetic rhetoric.
Condeming-Antisemitism (PDF)
Click on the above images to get larger view
![]()
Youth and Young Adult Resources
New Back to School Resources >> Click Here
NAMI Frontline Wellness Has Been Updated
NAMI Blog: Check out our recent blog post
“Loving Yourself After Psychosis: Healing and Moving Forward” in which author Sarah Ryan shares her journey to acceptance.
NAMI Launches First Podcast, “Hope Starts With Us,” Hosted by NAMI’s CEO Daniel H. Gillison, Jr.
![]()
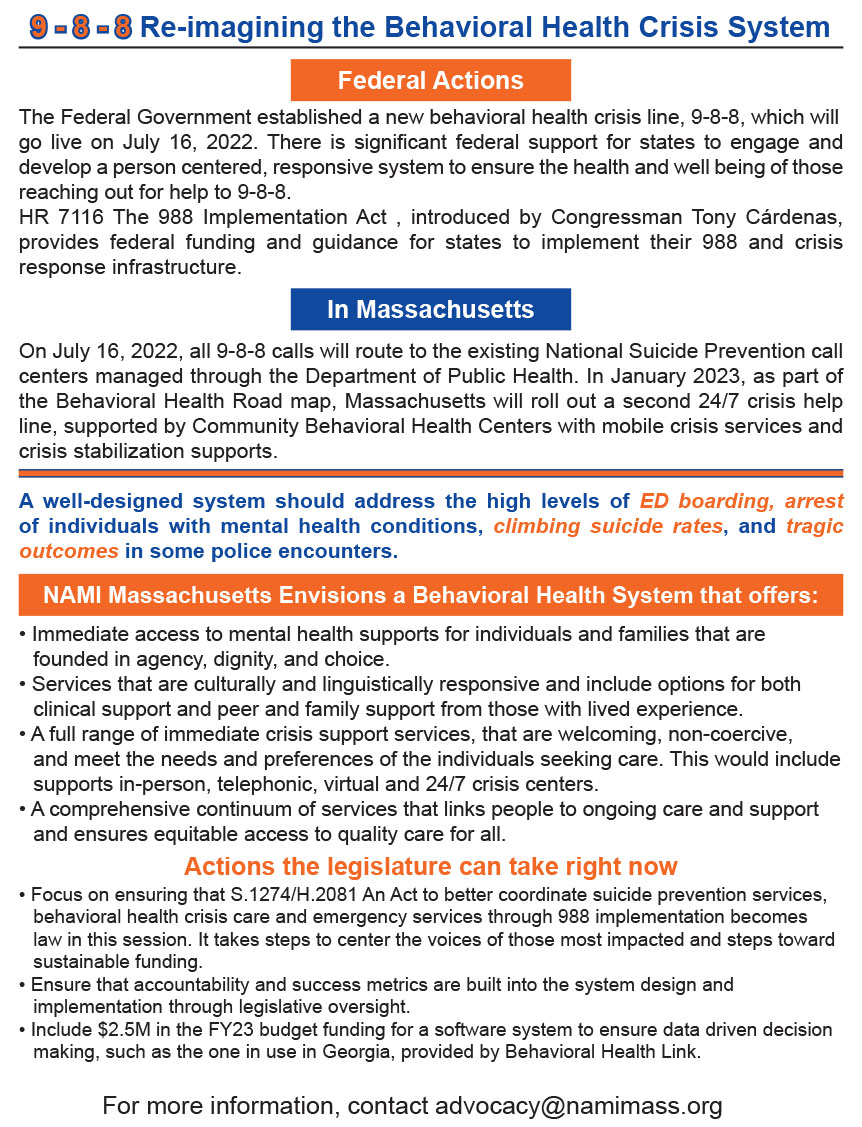
New NAMI Resources Around 988 >> Click Here
![]()
Please thank your state Representative and Senator for their dedication
to meeting the behavioral health needs of the people of the Commonwealth!


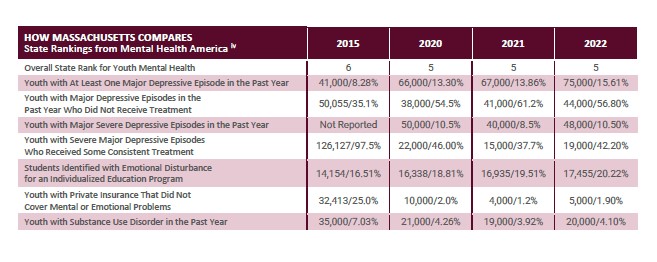
Massachusetts Ranked First for "State of Mental Health" - But Much Work Remains
Massachusetts was ranked first for its “state of mental health” in a new national report released this week by Mental Health America (MHA). The State of Mental Health in America report ranks each state according to the prevalence of mental health conditions and needs, access to mental health services, and barriers to access.
![]()
CMS NEWS: Biden-Harris Administration Awards $15 Million to 20 States for Mobile Crisis Intervention (9/20/21)

The recent tragic shooting of a woman by Saugus Police after her family called for help because she was experiencing a mental health crisis has again highlighted the need for change. NAMI Mass staff member, Tim Burton, and members of the NAMI Mass Board of Directors, Annabel Lane and Jennifer Paster, share their perspectives with WBUR. Click Here for article and audio.
NAMI Statement on Violence Against Asian American Community
![]()
NAMI Joined with the Harvard T.H. Chan School of Public Health for Virtual Panel Discussion: Mental Health in the Time of COVID-19
Moderated by: Jane Pauley of CBS
Panelists included:
- Daniel H. Gillison, Jr., NAMI CEO
- Dr. Ken Duckworth, M.D., NAMI Chief Medical Officer
- Chris Hubbard, Cleveland Browns NFL player and mental health advocate
- DeWanda Wise, actress and mental health advocate
- J. Corey Feist, co-founder of the Dr. Lorna Breen Heroes’ Foundation
- Dr. Shekhar Saxena, M.D., Harvard T.H. Chan Professor of the Practice of Global Mental Health
- Dr. Karestan Koenen, Ph.D., Harvard T.H. Chan Professor of Psychiatric Epidemiology

Podcasts Featuring Three Unique Perspectives on Serious Mental Illness Released in Partnership with APA’s SMI Adviser
In partnership with the American Psychiatric Association’s SMI Adviser, a SAMHSA-funded clinical support system for serious mental illness, NAMI is pleased to release the Medical Mind Podcast series led by NAMI Chief Medical Officer Dr. Ken Duckworth. The six-part series includes episodes on bipolar disorder, early psychosis and major depressive disorder.
Dr. Duckworth guides deep discussions of each condition that aim to offer insights for individuals, family members and mental health professionals, including: living with a serious mental illness, loving someone who has it, treating it, the impact of cultural identity and more.
For more details, click here.
NAMI Conducting Survey on Schizophrenia and Psychosis Conditions
NAMI is conducting an anonymous online survey to learn what participants think and what they know about clinical research on schizophrenia and related psychosis conditions, as well as what concerns they may have if they or a family member were taking part in a clinical research study. Survey responses will be used to help NAMI develop the most helpful information and support resources possible for people participating in upcoming clinical research study.
We are seeking adults with a diagnosis of schizophrenia, schizoaffective disorder, schizophreniform disorder or brief psychotic disorder and family members/caregivers of someone living with one of these conditions to take part in the anonymous online survey.
If you or someone you know is interested in participating, please visit our Frequently Asked Questions page.

New Year, New Data — NAMI Mental Health by the Numbers Update
NAMI is starting off 2022 with our annual update of Mental Health by the Numbers.
In 2019, 20.6% of U.S. adults experienced mental illness and 5.2% experienced serious mental illness. The number of adults with serious mental illness is now about 1 in 20, up from 1 in 25 in previous years.
As you raise awareness about mental health this year, make sure to check out the updated Mental Health by the Numbers webpage and infographics for the most current statistics on mental illness prevalence, treatment rates and more.

Covid-19 testing is still available. Find a location near you. >> ![]()
Download the special edition of our "Messenger" quarterly newsletter. It is loaded with useful information on support groups, covid-19 information and links to other useful programs and public health websites. Click Here>>
(Please allow a moment for the file to open)
![]()
![]()
Your #Vote4MentalHealth Matters
 NAMI Updates On The Coronavirus
NAMI Updates On The Coronavirus
COVID-19 And Mental Illness, NAMI Releases Important Information
COVID-19 guide for people with mental illness, their caregivers, and loved ones
Help people with mental illness in the COVID-19 crisis
NAMI hopes you and your family are staying well, and we recognize that the spread of coronavirus impacts every person in this country. But, we also know that people affected by mental health conditions face unique challenges during this time. We need your help to tell our nation’s leaders how they can support and protect people with mental illness.
As the Senate prepares the third in a series of COVID-19-related relief bills, please urge your Senators to ensure people affected by mental illness can maintain their treatment, get health and mental health coverage, access needed supports, and lift up the nonprofits they depend on, like NAMI.
![]()
Mauro Ranallo
Bipolar Rock 'N' Roller
Rated TVMA • 70 minutes
A raw and unflinching account of Mauro Ranallo's decades-long struggle with Bipolar Affective Disorder. The voice of WWE and Showtime Championship Boxing, Ranallo has called some of the biggest sports events in history - all the while fighting his own epic battles with mental health. Follow his journey as he combats the stigma behind mental health issues and sheds light on what it's like being at the top of the industry despite seemingly insurmountable odds.
Showtime/bipolar-rock 'n' roller
Watch the panel discussion from the 2019 NAMI National Convention in Seattle, with Dr. Kenneth Duckworth, NAMI Medical Director.
Panel Discussion on Bi-Polar Rock 'n' Roller w/Dr. Kenneth Duckworth and Mauro Ranallo

Watch the TED Talk Dear Stranger by Diana Chao; Youth Mental Health Advocate Diana Chao
Additional TED Talk by Youth Mental Health Advocate Diana Chao
Want to know what CIT is? Watch the Documentary Click Here>>

ORCHESTRATING CHANGE is the documentary film that tells the inspiring story of Me2/Orchestra, the only orchestra in the world created by and for people living with mental illness and those who support them. Co-founded by Ronald Braunstein, once a world-renowned conductor whose career was shattered when his own diagnosis of bipolar disorder was made public, the mission of the orchestra is to erase stigma one exhilarating concert at a time. As they rehearse, perform and prepare for a major concert, these extraordinary musicians have no idea how much the orchestra will change their lives in poignant and powerful ways.


NAMI Massachusetts has been asked by MassHealth to survey users of the Emergency Services Program. We are currently seeking individuals who have used the Emergency Services Program willing to take a 15-minute confidential phone survey. Your feedback is invaluable to improving the program. The information you provide is anonymous – your name will NOT be used.
To take the phone survey, please email LFDeAngelo@namimass.org
There are 21 ESPs serving communities throughout Massachusetts. The emergency services are available to help individuals having a mental health and/or substance use crisis and the ESP will come to your home or a school for example. They are alternatives to hospital emergency departments.
All ESP providers answer a toll-free 800 # and provide in-person behavioral health crisis assessment, intervention, and stabilization services 24 hours per day/7 days per week/365 days per year (24/7/365). Each ESP offers alternative settings in the community to hospital Emergency Departments (ED’s) for individuals seeking behavioral health services.
To find the ESP provider in your community click on the link below:
https://www.masspartnership.com/pdf/ESPflyerindividualsandfamilies.pdf
![]()

Money Does Not Equal Recovery: Bourdain, Spade, Cobain, and the Culture of Celebrity Suicide
By: Conor Bezane
-
A Road Map through the Criminal Justice System for Persons with Mental Illness and Their Families
Presented by NAMI Massachusetts
This guide is for people with mental illness, their families and their loved ones. In times of crisis, far too often families are uninformed and lose the opportunity to help prevent arrest, jail, and even prosecution, when their loved one is experiencing a psychiatric crisis. In these instances, what may look like wrongful behavior is really a symptom of their illness and a cry for treatment rather than criminalization.
View or Download the complete 70-page guide.complete 70-page guide.

NAMI Highlighted in Bedlam Documentary and Book
Bedlam, a full-length feature documentary produced and directed by Dr. Kenneth Paul Rosenberg, premiered at the 2019 Sundance Film Festival and will be released for wide distribution in April 2020. The film provides viewers a glimpse into the lived experience of people with mental illness who are unable to access appropriate treatment and support services.
The film’s companion book was released in October this year. NAMI is highlighted in the film, referenced on the film’s website and quoted on the book cover jacket. Bedlam offers opportunities to highlight key issues with stakeholders in your community and to advocate where NAMI is making an impact in communities across the country.
For more information about the film, visit http://www.bedlamfilm.com.
![]()
NAMI on Campus - Update Your Contact Information
In May, NAMI relaunched the NAMI on Campus initiative to NSOs and NAs with a simplified process for becoming an official NAMI on Campus club. Resources and marketing tools were updated for students looking to increase mental health awareness on campus.
For those currently working with a NAMI on Campus club, please complete a simple contact form to allow NAMI to communicate effectively with clubs and their points of contact. The form can be accessed directly here.
If you are interested in starting a NAMI on Campus club, please contact namioncampus@nami.org.
NAMI Partnership with HBO
NAMI recently kicked off a partnership with HBO which will feature a dedicated NAMI HelpLine number (1-833-HBO-NAMI) in all of its programming with content related to mental health/illness. Watch the video and read more about the initiative in Variety and the New York Times.
HBO has announced it will add mental health awareness “bumpers” ahead of select shows in order to identify specific mental illnesses that appear in the episode and provide a call to action for anyone seeking help.
The move comes as part of an initiative at the network called “It’s OK,” which aims to destigmatize mental illness and encourage conversation around mental health issues. Earlier this year, a report by the USC Annenberg Inclusion Initiative found that less than 2% of all film characters and roughly 7% of TV characters experience mental health conditions on screen, a failure to reflect the fact that close to 20% of the U.S. population reports some form of mental health condition or illness each year.
The premium cabler partnered with the National Alliance on Mental Health (NAMI) to create the warnings which are modeled on “The following program is rated…” slates that appear before movies and other shows. The list of series in front of which they will appear includes “Barry,” “Euphoria,” “Girls,” and “The Sopranos,” among others. Watch a short YouTube clip on OCD and "Girls"
NAMI Partnering with Kenneth Cole
Kenneth Cole, NAMI’s brand partner, is joining the mental health movement by initiating a coalition of creative influencers, game changers, fundraisers and NGOs. A future aim of the coalition is to fundraise directly for non-profits like NAMI.

Stop the Stigma: Why we need more conversations surrounding mental health See Video>>
Watch furthur video from the CBS report. More video>>
CBS NEWS October 9, 2019, 12:21 PM
NAMI Releases NFL Star Chris Hubbard “Strength Over Silence” Video
Docuseries Highlights Stories of Courage, Culture and Community View Video>>
NAMI Releases Video Series On College and Mental Health
NAMI has released a new video series aimed at helping college bound students and their families talk about mental health. The videos are part of the “Starting the Conversation: College and Your Mental Health” guide NAMI and the Jed Foundation released last year.
- See more at: https://www.nami.org/Press-Releases-and-media#sthash.7hKjmUBw.dpuf


Mental Health Conditions Seen In Childhood
Whether you are a parent, teacher, grandparent, aunt or uncle, our children are often our greatest pride and joy. They are our future. We love them, raise them, teach them, laugh with them, play with them and nurse them back to health. READ MORE>>

NAMI Releases First Free Online Class For Parents Of Children With Mental Illness
NAMI Basics OnDemand Adapts In-Person Course to Reach Nationwide Audience READ MORE>>

Six Myths And Facts About Mental Illness
The stigma associated with mental illness is now called “sanism.” Just like racism or sexism, it is a form of oppression and discrimination. And there is a lot of sanism and misinformation surrounding mental illness still present within our society. READ MORE>>
Engagement: A New Standard for Mental Health Care
To understand what effective engagement in mental health care looked like, NAMI invited experts, advocates and individuals with diverse perspectives and backgrounds to weigh in.
What emerged again and again was that to improve the lives of people with mental illness and their families, we must shift to a culture that embraces engagement as a new standard of care.
Top 10 Fitness Motivation Tips.
I was diagnosed with schizophrenia in 1987 when I was 22 years old. Taking medication and maintaining a healthy lifestyle has enabled me to achieve a better recovery and a better life; I have been living in recovery for over 28 years. So here are my Top 10 fitness motivation tips. These keep me on track and help me train for life. READ MORE>>
A Letter to My Colleagues About My Mental Illness
I still remember my first day of work after my psychotic break. I was so scared. I laid out all my clothes and took a shower the night before to be as ready as possible. I woke up extra early to have time to “just be ready.” My mental illness caused the psychotic break two years earlier. Since then, I have been rebuilding myself, overcoming a gauntlet of “first” fears. READ MORE>>
Promoting Mental Health at 30,000 Feet
About a week ago, I hopped on a Southwest Airlines flight in Denver, following NAMI’s annual Convention. I work remotely in Columbus, Ohio as a Senior Manager at NAMI, overseeing two of our education programs. Other NAMI members from Ohio were also on the flight and a member of the NAMI Ohio Board, Dave Morrow, happened to be wearing a NAMI cap and t-shirt. As we took our seats, flight attendant Lynda Lassiter recognized the NAMI logo and mentioned how much she appreciates all that NAMI does. As her captive audience prepared for departure, Ms. Lassiter announced that her son has a mental health condition and “without the NAMI Family-to-Family class,” she wouldn’t have known what to do. READ MORE>>
Tips For Adult Smokers with Mental Illness
Personal Stories: The Weather is Not Bipolar
So many people have equated the weather in my state with bipolar disorder. When it’s a high of 80 one day and snowing the next. I’ve fought this sentiment, because it negates the devastation of this serious illness. But I can see many ways in which extreme weather events are like mental illness. READ MORE>>
Showing What it Means to Have Bipolar Disorder
Comedian Believes that Mental Health is No Laughing Matter. READ MORE>>
Riding the Shark: Surviving Crisis/Catastrophe.READ MORE>>
![]()
Police Perspective: The Man in the Mirror
A dedicated police officer experiences intense psychological pressures of his job and learns that, as a cop,
your strength shouldn't be only physical. READ MORE>>
Hearts and Minds: NAMI Highlights Meditation, Yoga and other "Mindfullness" Practices for Mental Illness.
Mass Tragedies, Police and Mental Health: NAMI Releases Guide for Law Enforcement Leaders; "Preparing for the Unimaginable”

Video: “NAMI Ending the Silence” is a national mental health education program for high school students, based on real-life experiences.
"Ending the Silence" of Mental Illness in High School
Ask a Cop: What Should I Say When I Call 911 for a Family Member. READ MORE>>

Your Source for Regional Healthcare News & Information
![]()
Refer to our links page for more mass violence resources
![]()
Behavioral Health Coverage Under MHPAEA
A Nationwide Expansion
Do you have questions about what your health insurance covers for mental health or substance use disorder services?
The Mental Health Parity and Addiction Equity Act (MHPAEA) of 2008 requires health insurers and group health plans to provide the same level of benefits for mental and/or substance use treatment and services that they do for medical/surgical care.
The final MHPAEA regulations published in 2013 applied parity protections to the commercial market, and final regulations issued by the Centers for Medicare & Medicaid Services on March 29, 2016, applies parity rules to Medicaid managed care and the Children's Health Insurance Program. As a result, parity requirements now apply to most health plans in the United States.
Download these resources about parity for mental health and substance use disorder benefits:
Know Your Rights: Parity for Mental Health and Substance Use Disorder Benefits

![]()
5 Famous Females Who Are Crushing The Stigma of Bipolar Disorder
By being public about their bipolar, these celebrities help others to understand the brain-based disorder.
#1 Jane Pauley Photo: NBC Universal Television
Photo: NBC Universal Television
![]()


7 Ways to Manage Depressive Thoughts
Here are seven techniques that can help you improve your mood when living with depression.
Belief that things can change for the better is called hope, and it’s crucial to living well with bipolar disorder.
Integrating mental health and primary care
Integrating Mental & Physical Health Services Through Primary Care Teams Results in Better Outcomes & Lower Costs, New Study Finds
Esperanza Magazine:

Mom to Mom: 5 Ways to Get Through Depression and Guilt
![]()
15 Ways To Support a Loved One with Serious Mental Illness - READ MORE>>
Pulitzer Prizes represent the highest honors for print journalism. They are given in recognition for both professional excellence and public service.
This past month marked the 100th anniversary of the awards. What is even more exciting is that several selections focused on mental health concerns, bringing attention and awareness to the movement.
- See more at: http://www.nami.org/Blogs/NAMI-Blog/May-2016/These-Take-the-Prize-Journalists-and-Mental-Healt?utm_source=naminow&utm_medium=email&utm_campaign=naminow#sthash.PbTTf3XX.dpufPulitzer Prizes represent the highest honors for print journalism. They are given in recognition for both professional excellence and public service.
This past month marked the 100th anniversary of the awards. What is even more exciting is that several selections focused on mental health concerns, bringing attention and awareness to the movement.
- See more at: http://www.nami.org/Blogs/NAMI-Blog/May-2016/These-Take-the-Prize-Journalists-and-Mental-Healt?utm_source=naminow&utm_medium=email&utm_campaign=naminow#sthash.PbTTf3XX.dpufPulitzer Prizes represent the highest honors for print journalism. They are given in recognition for both professional excellence and public service.
This past month marked the 100th anniversary of the awards. What is even more exciting is that several selections focused on mental health concerns, bringing attention and awareness to the movement.
- See more at: http://www.nami.org/Blogs/NAMI-Blog/May-2016/These-Take-the-Prize-Journalists-and-Mental-Healt?utm_source=naminow&utm_medium=email&utm_campaign=naminow#sthash.PbTTf3XX.dpufPulitzer Prizes represent the highest honors for print journalism. They are given in recognition for both professional excellence and public service.
This past month marked the 100th anniversary of the awards. What is even more exciting is that several selections focused on mental health concerns, bringing attention and awareness to the movement.
- See more at: http://www.nami.org/Blogs/NAMI-Blog/May-2016/These-Take-the-Prize-Journalists-and-Mental-Healt?utm_source=naminow&utm_medium=email&utm_campaign=naminow#sthash.PbTTf3XX.dpufPulitzer Prizes represent the highest honors for print journalism. They are given in recognition for both professional excellence and public service.
This past month marked the 100th anniversary of the awards. What is even more exciting is that several selections focused on mental health concerns, bringing attention and awareness to the movement.
- See more at: http://www.nami.org/Blogs/NAMI-Blog/May-2016/These-Take-the-Prize-Journalists-and-Mental-Healt?utm_source=naminow&utm_medium=email&utm_campaign=naminow#sthash.PbTTf3XX.dpufPulitzer Prizes represent the highest honors for print journalism. They are given in recognition for both professional excellence and public service.
This past month marked the 100th anniversary of the awards. What is even more exciting is that several selections focused on mental health concerns, bringing attention and awareness to the movement.
- See more at: http://www.nami.org/Blogs/NAMI-Blog/May-2016/These-Take-the-Prize-Journalists-and-Mental-Healt?utm_source=naminow&utm_medium=email&utm_campaign=naminow#sthash.PbTTf3XX.dpufPulitzer Prizes represent the highest honors for print journalism. They are given in recognition for both professional excellence and public service.
This past month marked the 100th anniversary of the awards. What is even more exciting is that several selections focused on mental health concerns, bringing attention and awareness to the movement.
- See more at: http://www.nami.org/Blogs/NAMI-Blog/May-2016/These-Take-the-Prize-Journalists-and-Mental-Healt?utm_source=naminow&utm_medium=email&utm_campaign
![]()
Office of the Attorney General Establishes a New Hotline to Report Threats and Harassment
Our job in the Attorney General's Office is to protect people's rights, fight discrimination, and keep people safe. In recent weeks, we've seen reports from around the country and our state of harassment and intimidation of racial, ethnic and religious minorities, women, LGBT individuals, and immigrants. Such conduct runs against our values as a society, and we are acting to ensure that our residents are protected.
In just over two weeks, our Office has received over 400 calls from the public reporting issues of hate and harassment. As you might know, Attorney General Healey established a new 1-800 hotline for residents to report bias-motivated threats, harassment, and violence managed by attorneys and staff in the AG's Office. The hotline number is 1-800-994-3228.
The Attorney General's goal is to make it as easy as possible for residents to contact us. Any Massachusetts resident who has witnessed or experienced bias-motivated threats, harassment or violence may call the Attorney General's hotline or fill out a civil rights complaint form at this link. Residents may also contact the AG's Office through our Facebook and Twitter.

Article from the Social Security Administration: When People Need Help Managing Their Money
Article from the Social Security Administration: Plan to Achieve Self-Support (PASS)
https://www.socialsecurity.gov/disabilityresearch/wi/pass.htm
Click the image below for the Mass.gov Department of Health and Human Services
Article: Cash Assistance in Massachusetts. READ MORE>>
Office of The Secretary of The Commonwealth of Massachusetts: CLICK HERE>>
A Police Officer Who Did The Right Thing: Helped My Son When I Couldn't

By Laura Pogliano on the Pete Earley blog
My 22 year- old son, Zac, has schizophrenia, the paranoid type. Since February, he has phoned emergency services five times to ask for help for problems that he's imagining. Sometimes it's a heart attack, sometimes his throat is closing, and yesterday, it was to report a gunshot wound to his head. Read More>>
Article appears in New Scientist: READ MORE>>


